
A systemic view on the Corona-crisis revisited by BCSSS Vicepresident Felix Tretter
A SYSTEMIC VIEW ON THE CORONA-CRISIS
Felix Tretter, Vicepresident, BCSSS, (April 25th, updated on December 3rd 2020)
Revisited Preface
Now in fall 2020, I think it is time to review lessons learned from CVOID-19 crisis. Facing the beginning Corona pandemic in spring 2020 I tried to identify topics for analysis and management of this crisis where systems thinking could be the insightful approach. At first, I claimed for a wide and systemic socio-ecological framing regarding the basic eco-systemic view of the virus in the living world and I argued for careful application of numbers and equations to capture the dynamics of the epidemic / pandemic. I framed my considerations with a public health perspective, and finally I introduced briefly into the importance of systemic modelling in epidemiology. I finally proposed an (organismal) “systems medicine” in the sense of Ludwig von Bertalanffy and suggested further exploration. In this update these paragraphs are repeated (Part I), and in a second section, Part II, I refer to the current situation in fall 2020.
Part I – the pandemic in spring 2020 (April 25th)
The so-called “Corona-crisis” is a shocking reset-push for the global society. Fundamental nature-humans relations that up to now seemed to be controlled by technology and society are currently disrupted by this “communicable disease”. With other words: the ecology of humans is worldwide under shock. Mainly long-distance travelling with local spreading clusters transformed a local epidemic in China to a pandemic within only a few weeks.
In many aspects health authorities and public policy agencies underestimated the dynamics of the Covid-19 virus, regarding its contagiosity, pathogenicity and lethality – some of them reacted very late and implicated hundreds and thousands of deaths. Other authorities probably overdosed public order by sudden and severe restrictions. Now, in the end of April 2020, citizens of many countries have to live under restrictions of social order by politicians who are held responsible and who completely rely on predictions of medical experts and their data-based mathematical simulations. We all hope for successful medications and vaccinations this fall, but it seems it takes a longer time and that we have to accept partial lock-down for a longer period.
If we want to establish and strengthen a society based on the ideals of a humanism, citizens should be able to comprehend and also criticize and deliver backgrounds of political decisions. In line with this, we think that a better understanding of the dynamics of epidemics and its coping procedures might be possible by systems thinking as it was proposed by Ludwig von Bertalanffy [1] and his colleagues.
The population and the viruses are living systems
Living systems are environmentally embedded and they exhibit significant self-organized dynamics. For better understanding, a systemic ecological framework can be useful. Current approaches in human epidemiology even apply dynamics similar to predator-prey relations for understanding spreading of communicable diseases and their suppression: the analogy applies as the virus potentially destroys the host, because the host falls ill, but the host also produces antibodies that inactivate the virus. This type of agonist-antagonist dialectics in population dynamics was highlighted by von Bertalanffy referring to the nonlinear Lotka-Volterra differential equations on predator-prey models in demecology.
Mathematics and data are needed for public affairs
The data on the number of infected individuals observed by the health care system (public health) showed very soon and for some weeks features of exponential growth (e-function) promising an explosion of this comparatively highly lethal virus. Regardless of the quality of measurement of the data (selectivity, reliability, validity, sensitivity, specificity, report delays etc.), recorded daily new infections were plotted, logarithmic transforms were displayed, reproduction numbers and doubling time as indicators for political decisions were explained publicly etc. So, the whole population of the world, if interested, had a crash course in applied math, with regard to fitting data and understanding non-linear dynamics of living systems and their epidemiology.
The need for intervention and policy evaluation – how to suppress epidemic dynamics and what is the systems response?
Exponential growth evoked public order reactions to dampen the dynamics. Several public order interventions intended to “flatten” or even “hammer down” the curve, namely by social distancing, disinfection, quarantine, lock-down of shops and markets etc. And after some weeks of general lock-down a sigmoid growth curve could be identified, similar to the Bertalanffy growth function that he developed for mass growth of animals. The main question was: Which measure is the best indicator for policy success? The doubling interval of prevalence, the reproduction number (how many individuals are infected by a single individual within a certain period) etc.? And finally: How strong is the delay of the display of data referring to the time they were collected. Are the tests sensitive and specific enough? So: Is the data base robust to justify political decisions that potentially collide with human rights and economic interests? In early stages of the pandemic only a few understandable articles appeared that addressed these problems of understanding the dynamics and designing regulations [2].
Now some countries succeeded in suppressing the dynamics and they reduce the lock-down. However, the measures mentioned above must be observed in order to avoid a “second wave”. This is a dance on the tightrope.
From a systems analytical view, the policies can be seen as a set of inputs into a dynamic self-organizing multi-level system where the crucial problem of multivariate statistical analysis is: Which of the observable changes in the data (and derived indicators) of the system’s state is a “specific differential response”, and which not and how can we distinguish these from each other?
Methodology of modelling in “Systemic Epidemiology” – mathematics alone is not a theory
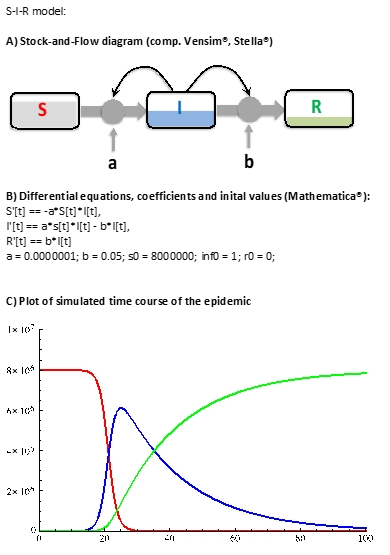
Now in some countries, like in Austria, the sigmoid curve goes down to the baseline, corresponding to the declining components of the I-curve of the basic SIR-model, where S stands for the population subgroup of susceptible persons, I stands for the infected persons and R indicates the number of recovered persons. This model is the core model of the model pool of systemic epidemiology [3], a field that helps to constitute Integrative Systems Medicine as we aim it in BCSSS [4] [5] (s. Fig.1). It usually is extended to a SECIRD model depicting exposed persons (E), carriers (C), deaths (D) etc. The main “flow” of persons between these compartments from S over I to R can be modelled regarding empirical data that indicate transition velocities. Differential equations describe these flows and stocks formally, but the model can be visualized qualitatively by boxes and arrows diagrams, for instance based on the technique of Systems Dynamics. This methodological modeling procedure – from concept to diagram to equations to simulations – is very useful in inter- and transdisciplinary communication, especially in this heterogeneous crowd of medical experts – a picture says more than thousand words (Fig.1).
The need for integrated multidisciplinarity and transdisciplinarity in medicine (and not only there)
Analysis of and coping with corona crisis is provided by virologists, laboratory experts, infectiologists, epidemiologists, immunologists, pharmacologists, pulmonologists, intensive care doctors, public health experts, general practitioners, and other medical experts. Although most have an education in medicine, there is a lack of a field like “theoretical medicine” that integrates the different aspects and view points on a conceptual level, that bridges different islands of health knowledge and that reduces avoidable conflicts and enhances coherence in analysis and action.
Regarding this need for integrative viewpoints, systems thinking has a strong power for interdisciplinary integration as it was demonstrated by Ludwig von Bertalanffys General Systems Theory”. As mentioned above, in the BCSSS we try to bridge these knowledge gaps by our international and interdisciplinary working group on Integrative Systems Medicine.
Further tasks – an integrated view on control of the pandemic
At first, a differential evaluation of public order interventions has to be done to prove the effects of specific public health and public order interventions and to eliminate ineffective and freedom-reducing regulations. Of course, also effects on economy and psycho-social disturbances must be included in this view. In consequence, the above described multiplexity of the corona pandemic demands further exploratory modeling by models that include economy, psychosocial variables, etc. Methodologically, this analysis and regulatory aims need much caution and relativism. BCSSS plans to organize such a live-workshop if public health measures will allow it.
But also, further issues are challenged by corona pandemic, namely the current culture of economy, law, science, social order or briefly: the structure and function of the our human ecological system.
In summary, we think that application of and education in systems thinking could provide a tool for integrative viewing of dynamic processes like this pandemic. Not only medicine but also economics, psycho-social issues and other factors could be considered similarly to the famous world models [6].
Part II – WHERE ARE WE NOW (December 2020)?
Now in December, about eight months later, I want to add some issues for progress in the systems view of Corona with focus on Austria, Germany and Europe. At first, I want to mention that the BCSSS organized several meetings on COVID-19 with focus on medicine, some results were published in German (Tretter u. Adam 2020 [7]). Also, a video-meeting on systems medicine with reference to COVID 19 was arranged. A publication informed by these meetings is in preparation.
In this text, I want to present some features of systems thinking as I understand it. Then I conceptualize COVID-19 management within a basic system theoretical framework and finally I make a sketch of a systems pathology of COVID-19. Some of these issues were discussed already in part in a German publication series on “Corona-future-management”.
Methodology of systems thinking
Since Ludwig von Bertalanffy the art of systems thinking developed as a culture to think about phenomena and to influence them especially in organizational contexts (Checkland1981 [8], Midgely 2000[9], Maani & Cavana 2000 [10]).
Basically we think that a “transdisciplinary” problem definition and its solution is the most appropriate approach for solving complex problems as it was developed practically by sustainability research ( Scholz 2011 [11], Ison 2020 [12]).
In this context, the basic assumption is that the world is a complex dynamic system consisting of a large number of horizontally and vertically coupled subsystems as J.G. Miller and other systems thinkers suggested (Miller 1978 [13]). In addition, we think some kind of a constructivistic epistemology is appropriate as the virus can only be detected by sophisticated measurement technologies. The concept of the virus per se also depends strongly on the method of study: virologists use electron microscopes, epidemiologists use data obtained by laboratory tests (polymerase chain reaction test; PCR test) or serological tests that show that at least 2-times more persons exhibit anti-bodies than were tested positively by PCR-tests because they had symptoms. This indicates that in case of infection about 50 percent of infected persons are asymptomatic, even if the methodological situation is complicated: this indicates that the epidemiological numbers and indicators are constructs. In consequence, the communication of the CVOID-19 problem is a co-construction of this problem and not simply the “reality”. In other words, the reality is finally a mental model of the outer world.
The relevance of the mental model of the world within an action cycle and for a deeper understanding of the causal mechanisms is reflected within the Systems dynamics method of modelling (Sterman 2000 [14]). Regarding COVID-19 to be a public health problem one could refer to John Sterman who stressed the point that unintended side effects can counter-balance the problem (Sterman 2006 [15] ). Also Gerald Midgley proposed systems thinking and intervention in public health issues where he emphasizes (1) the need to explore stakeholder values and boundaries for analysis, (2) problems of marginalization, and (3) a wide range of methods to create a flexible and responsive systems practice (Midgley 2006 [16]).
The construction of models for orientation for action
For construction of a systems model it is useful to start with a list of characteristics of the system without considering the interactions. In a next step the causal relationships should be checked between the individual factors. With this goal, the factors x1 to xn that cause the respective factor y should be identified, as well as the effects of the factor y and its collateral effects z1 to zm should be explored. By this procedure, an influence matrix can be constructed. In many areas – such as the management sector – only qualitative or semi-quantitative observations are available for this purpose, so that in consequence only qualitative modelling is possible, which can also be used for process control. It is therefore important to push ahead with quantification. The reverse way, however, that the data are differentiated and / or aggregated by use of tools of multivariate statistics (variance analysis, discriminant analysis, factor analysis, cluster analysis etc.) implicates somehow plausible interpretations of the results without reference to any specialized theory. This procedure is typical for multivariate analyses, especially in big data projects und it often turns out to be an epistemically unsatisfying project.
However, on the basis of such models, the phenomenology of the dynamics of the epidemic / pandemic as well as the differential effects of health care and public health measures can be explored more in detail.
Medical care – many counterproductive actions
In the view of General Systems Theory and its concept of “flow equilibrium” (Fließgleichgewicht, L.v. Bertalanffy) phenomena of interest should be seen as systems states that fluctuate around an equilibrium point. The level of these system states are supposed to be the result of activating and inhibiting forces. Regarding this, the indicators of Covid-19 epidemic/pandemic can be seen as results of presence and invasivity of the virus as “drivers” and protective behavior and mechanisms of the population as “brakes” of the dynamics of these numbers.
During the first wave in Europe in spring 2020, the supply system has played an important suppressive role against a malicious dynamic, at least in preventing fatal outcomes. It begins in the outpatient sector, with telephone services (e.g. Corona-Hotline), then with the pharmacies and the general practitioners / family doctors / practitioners. They are the gatekeepers of the care system. Above all, facilities such as the Covid info phones, which then arrange for outpatient testing if necessary, are new constructions whose efficiency is still urgently to be clarified. They have a decisive effect on patient flows.
However now, in fall 2020, it becomes apparent that the authorities in some European countries have probably not paid enough attention to recruiting enough qualified personnel or to creating enough jobs for contact tracing. In spring 2020, the employees of the clinics and their intensive care units had to work to the point of exhaustion and so far, they have had far too little to say. They often served only as illustrations for the messages of the media. After public praise for the work, however, there was little concrete reinforcement of the system by politics and the state. It is important to note that also financial boosts for health care are not enough because the acquisition of personnel is not so easy as the conditions of work are not so attractive. Also, the health care system is increasingly being structured, organized and controlled according to business criteria and less according to medical aspects, which might result in poor process quality (Tretter 2000 [17]; Tretter 2005 [18]; Tretter 2011 [19]). Before all, there is an urgent need to revise the economization ideology of New Public Management in the public sector (Schedler and Pröller 2011 [20] ) and to implement the possibly more human-centered culture of New Governance (Tretter and Welpe 2018 [21]). This is indispensable for the management of structures of public administration whose function is to help people, i.e. when living systems work for „living systems“. Many young people who work or want to work in the health care professions are deterred by the structural working conditions despite their high motivation, while a high percentage of older medical employees are close to burnout (Deutsches Ärzteblatt 2020b [22] ).
The evaluation of damping measures – a problem of complexity
For the success of the handling of COVID-19 it is difficult to justify which target indicators, and which mix of them, should be used as outcome variables: the number of tests/million inhabitants, the cumulative infection numbers, the rate of change of the daily newly infected, the weekly incidence of < 50/100,000 inhabitants, the mortality, the lethality, or even the gross national product, since it is a question of the overall social effects. The variables that determine the outcome, such as the extent to which people are required to wear masks, freedom of movement, regulations for public spaces, but also access to medical care structures, etc., would then have to be integrated into a multivariate equation, in which, for example, the number of newly infected people y is seen as a result of the effectiveness of risk factors x1 to xn minus the protective factors z1 to zm . If these relations would be made more explicit and the variances and covariances of these variables would be examined in regional and international comparison a better guideline for public health regulations would be possible. However, data analyses without theory are inadequate; they require a foundation of stratified mechanistic social-epidemiological models that appropriately reflect the epidemic dynamics on the basis of socio-structural variables (class, lifestyle, milieu, etc.). Urban analyses would also contribute to a differential understanding of the effectiveness of measures.
Although such multivariate equations formally appear in data-driven modelling, they are not publicly discussed in terms of their theoretical interpretation in context of social sciences. However, it has already been made clear on several occasions that the available epidemiological data are of fuzzy quality, because of low reliability and validity that make it difficult to monitor and evaluate the efficacy of the prevention measures. Even big-data analyses such as they were published by some research institutes cannot compensate for this, especially since they hide these methodological shortcomings and are not based on a theoretical framework (Antes 2020 [23]).
Also with regard to individual measures, for example, the recommendation, and later the order, to wear a mouth and nose mask has a tradition of over a hundred years and is certainly proven. Wearing masks when shopping and other activities has become a common practice in high-density areas and especially in small towns and seemingly has protective effects at communicable diseases. However, the scientific basis of effectivity of those masks, which fulfils the criteria of evidence-based medicine, is weaker for the COVID-19 pandemic than one might think, because there are only fragments of evidence that make the benefit of the masks plausible, such as simulation studies, laboratory tests with COVID-19 patients, etc. (EbM Network 2020b [24]).
However, a strong preventive effect is generally attributed to the prohibition of large events, especially indoor events. The closure of kindergartens and schools remains a controversial issue: The children are possible spreaders, but they hardly get sick themselves. Some studies show positive effects of school closures, some do not. Home quarantine is plausibly effective.
If one still tries to consider the dynamic aspect, namely that both the drivers of the epidemic/pandemic (which are unknown at least in their effectiveness) and the prevention measures as brakes vary, then the certainty of knowledge is shaken once again. It is precisely the dynamics aspect that advises a systemic perspective, namely, to represent the epidemic and its control in a control loop model, i.e. conceiving it as an operationally closed system.
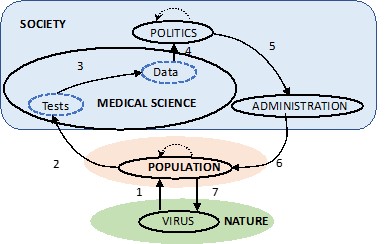
Control loop model of the COVID 19 management – systemic management
Applications of system models in management practice of the COVID 19 problem could serve for self-reflection of the intervention and for reorganizing insufficient structures: The cycle – virus presence, population infection, testing, epidemic data, political regulations, enforcement by authorities, population behavior, changed virus exposure, new testing or data, etc. – is in fact a control loop that is driven by the relationship between the set points of politics and the actual values (and forecasts) of science. This control loop is – as has been shown before – fundamentally characterized by the problem of reaction delay. From the point of view of system theory this property can lead to chaotic processes due to under- and over-regulation, i.e. a control failure due to an unconsidered „delayed response“ (Dörner 1997) [25]: As has been shown, the data for the political decision are already eight days old, the implementation of regulations also takes a few days, and until the change in the epidemiological figures occurs due to changes in population behavior, again eight days have passed, etc. (see Fig. 2). In result, the stimulus-response delay extends from two to three weeks! However, the infection doubles within a few days! This is particularly problematic if politics is mainly based on a science that is “data-driven” and thinks only in quantitative and static terms and whose prognoses are burdened with considerable variance instead of using theoretical reasoning to proceed in understanding the dynamics of the pandemic. This kind of data-centered formal thinking urgently needs support by content-related social sciences!
In consequence, the key to the efficiency of control of COVID-19 pandemic lies in the political and official problem management, which needs to be examined urgently in order to detect and reduce unintended side-effects. The dominating control loop model is grounded on a management concept that is typical in business administration and which is based on a machine model that assumes a simple input-output model of the population without considering and respecting the intrinsic dynamics of the respective components as they are typical for living systems. From a systems theoretical perspective, a biosystemic management concept and a corresponding practice are therefore more appropriate.
Systemic management
Systemic management is based on the assumption that firms are living systems, at least because they are realized by humans for services to humans. According to this, organizations – e.g., government agencies, businesses, supply structures, hospitals – should already correspond in their functional and structural design to the multi-level structure of the nervous system (e.g., spinal cord, cerebellum, cerebrum) (Beer 1972 [26], Malik 2016 [27]).
In addition, management practice in the fulfillment of tasks (e.g., ensuring public health) should be employee-centered, and implement operational goals in a dynamic and balanced score card system, in which at least the concerns of clients, those of employees, process quality and, of course, finances are differentiated, but assessed in the context of the overall picture (Tretter 2011 [28]).
A major problem of the social COVID 19 management is still that the many causal loops are coupled into this basic process and therefore also influence it – a network of components must be considered.
Therefore, it makes sense to use not only a data-driven model of the socio-ecological system to be regulated, but also a content-based model of the system to be regulated. A socio-ecological model consists of two subsystems, namely society and nature, whereby „society“, as mentioned at the beginning, consists of a set of social subsystems, sometimes including the population. “Nature“ refers to natural ecosystems, such as primeval forests, with plants and animals, but also soils, water and air. However, the human civilization program of humanizing nature leads to the fact that nature is regarded as an endless resource without assigning it an intrinsic value. This leads to overexploitation and the careless penetration of natural systems by human systems. In this context, zoonoses are of concern for COVID-19, i.e. infectious diseases that can be transmitted from wild animals to humans (and vice versa). These diseases have already caused many epidemics and are probably the origin of COVID-19. Especially viruses such as Ebola, smallpox and some influenza viruses have already cost the lives of a large number of people. The malicious thing about viral zoonoses such as SARS-CoV2 is that there is no adequate therapy and prophylaxis for these and many other viruses for a longer time. More thoughtfulness is needed here.
Collateral Effects
The COVID-19 control loop described above is embedded in a variety of social systems on which this control process has an impact, and which also have a retroactive effect, thereby further complicating this control process and generating process disturbances, no matter how much they appear justified from the point of view of the respective subsystem actors (e.g. chamber of commerce, mass media, social media etc.). This is generally referred to as „collateral effects“ and „constraints“. The basic methodology of system theory of zooming-out for the identification of the described control loop and zooming-in for component analysis results in a systemic network model, which is explained in more detail below.
The perception of the corona problem within medicine and the recommendations for action that were communicated to politicians and, through the media, to the population, has led to a dampening of the epidemic dynamics through lockdown measures. However, the lockdown clashed with the goals of economy, law, education, culture and ultimately, in general, the assurance of a „good life for all”. In consequence, the state was (and is for the time being) subjected to a complex and varied stress test.
In addition, some highlights are to be mentioned here, above all the conflict between ethics, which medicine demands, and the justified interests of the economy, whose collapse would be „unhealthy“ in other ways.
Economy
The aim of the economy is to secure the cyclic money flow or to accelerate it. However, the lockdown almost brought the cycle to a standstill. Politicians initially in spring argued that many deaths could be prevented, and that health care would not be overloaded. However, at the end of April, the business community was increasingly saying that the profitability of many companies was no longer guaranteed and that employees would have to be laid off.
In essence, this conflict between medicine and business means that one prevented death or one life saved (LS) results in dozens or even hundreds of company closures and thus a large number of unemployed (UE). An explication of such a cynical but implicit equation in the public perception is:
y LS = x UE (e.g. 1 LS = 10 UE or 100 UE etc.)
A health or insurance economist could now go further by depersonalizing this equation and transforming it into Quality Adjusted Life Years (QALY) or Values of Safed Lifes (VOSL) and expressing it in monetary units (Conover 2020 [29]). Assuming that an unemployed person „costs“ about 13,000 Euros per year, a saved life would then be worth 130,000 Euros or perhaps 1.3 million Euros, an amount that is also assumed by life insurance companies. Without going into further detail here, the basic relationship between health and economy is at stake. With this comparison, one can see, whether one likes it or not, that such decisions fundamentally challenge socially supported ethics. This also applies to the law system.
Law
Several areas of rights are negatively affected by a lockdown: First of all, the individual right to freedom of movement etc. guaranteed by constitutional law, which ensures free movement, travel, etc., is at stake. However, the liability law interferes with a self-inflicted situation if a trip was made despite travel warnings for a country and then there are difficulties. In this case, also tour operators are in obligation. If authorities fail to initiate hygiene measures, then they too are confronted with liability lawsuits and even criminal lawsuits from sick visitors, as is currently being tried in court for the town of Ischgl in Tyrol. Labor law is also affected, in so far as the duties and rights of both the employer and the employee are unclear with regard to home office. Linked to this is the data protection law, which is also being questioned. Finally, the overriding goal of public health comes into play in the case of violations of regulations provided for by the law of order (prohibition of entry).
The mention of these few areas of law already shows the broad scope of the protective and restrictive positioning of medicine with regard to the corona crisis and also the imposition on legislators to reflect life in even greater detail in legal texts. Finally, the courts are also concerned with the „proportionality“ of measures, where court proceedings with corresponding expert opinions are still pending. The question is therefore above all how the individual person is positioned in relation to the community.
As mentioned, all areas of society are ultimately affected by the COVID 19 pandemic, and this in an interwoven relationship. For a more detailed but comprehensive understanding, especially for the near future, a social and ecological perspective is needed, in which the health problem is one of many others. This perspective is increasingly referred to as the socio-ecological perspective.
A socio-ecological perspective – besides the COVID 19 crisis there is the climate crisis
In view of the fact that SARS-CoV2 originates from wild animals, i.e. from natural ecosystems, it should be more comprehensively thought about the social relationship to nature consisting of the relationship system nature-human-society. This view is typical for the interdisciplinary perspective of „human ecology“ or „social ecology“ (Serbser 2004 [30]; Fischer-Kowalski et al. 1997 [31]; Becker u. Jahn 2007 [32]). This research approach analyzes socio-ecological systems and can provide both analytical achievements in penetrating the interdependence of sustainable development goals and corresponding orientations for action (Sustainable Development Goals; EU 2019 [33]). The feasibility of the 17 SDGs in the course of a sustainable development of the world society is examined in a transdisciplinary and interdisciplinary framework as a socio-ecological system.
To illustrate the central challenge in the field of SDGs, one need only think of the tension between ecology, economy and social issues, which became popular through „Fridays for Future“ and other critical social events in 2019. The issue of climate change and its „drivers“ – energy production, transport, etc. – and the economic and social frictions of change, was demonstrated by the resistance in France to new fuel prices in the sense of an „eco-tax“. These aspects are particularly important in the course of the reorganization of the now disturbed economic order. The connection between the goals of health (SDG #3) and poverty reduction (SDG #1), food security (SDG #2) and education (SDG #4) also needs to be examined more closely. Synergies of political action are therefore required, even if the initial focus is on COVID-19!
With such a comprehensive systemic socio-ecological perspective, as addressed by EU Commission President Ursula von der Leyen with the „Green Deal“ (EU [34]), even the simple input-output model of the COVID-19 pandemic and its management needs to be revised. This especially in view of the low process quality and efficiency of the prevention measures. The subsystems and processes involved can first be listed according to the methodology of systems science in line with the real sequence of events and then presented as a closed loop model (see Fig. 3). Starting from a general level of the conceptual framework model of human ecology, namely the interaction of nature, population and society, COVID-19 is a serious problem, but only one area of the present society: The virus, originating from a natural ecosystem, invades the human population (POPUL; 1a). A relevant risky exposure behavior of the population occurs (1b).
Sick parts of the population make demands on the health care system (HEALTH C. 2a). Medical science (MED-SCIE) identifies the epidemic and its causes (2b). Science communicates this to politics (3a). The media (MASSMED) recognizes the scientific discourse (3b). The health system reports the situation to politicians (3c). Politicians publish the situation and announce measures (4). This is repeated (4′). The mass media communicate this perspective to the population (5). This is repeated (5′). Politics formulates (epidemic crisis) laws and regulations (6). This is repeated (6′). These laws are issued to state organs (administration, authorities, schools, etc.) and to the economy (ECON; 7a, 7b, 7c, 7d). The state (see above) implements and controls (8). School closures affect families (9). The economy is now suffering (10). The economy is gradually intervening more intensively in politics (11). Cultural standards shape the behavior of the population and thus influence politics, vice versa (12 a,b).
Science is gradually developing technologies (TECH) for diagnosis and therapy and prophylaxis, though partly as a future option (13). Technology (e.g. vaccination) helps the population and stops the virus and epidemic (14 a,b).
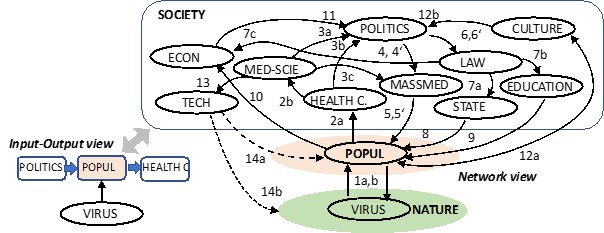
Simple Input-Output Model:
A –> –> –> –> –> –> –> B
A further elaboration of this system perspective, considering all relevant interactions, would emphasize the network aspect and specify the strength of the relationships and especially the time relations. To increase the validity of the model, this would have to be „transdisciplinary“, as explained above. But where does the human being remain in the system, for whose welfare the entire emergency mode is organized?
Humans as the center of society
The COVID-19 measures focus on the common good of the population however individuals, even as groups, are out of sight. From a humanistic perspective, which was also an aim of Ludwig von Bertalanffy, also the individual human should be of central interest.
The „situated subject“ – the Ecology of Humans
The harsh collective lockdown throws people back to their „home“, their oikos. Some are in privately owned homes, others in a nursing home, quite a few are homeless. After weeks of isolation and the continuing danger of a repetition of this situation, zoon politicon is deprived of an essential dimension of human existence, namely the social, especially considering that about 40% of people live in single households.
This forced individualization can partially be compensated by digital communication technologies, but the duration of this situation can lead to mental changes, and always with a potential for illness. This process of loneliness can also be found in families that are isolated by lockdown (“together lonely”)!
These psychosocial dimensions of the pandemic and its management are only rudimentarily researched, but they are already evident in psychotherapeutic practices. Besides the dissatisfaction of social needs for relatedness, acceptance and binding, the lockdown conditions can lead to further perturbations of basic needs such as those for existential security and individual freedom and self-development.
This also applies to the attitude to life of young people, who statistically feel less at risk and, with increasing duration of the restrictions, have a growing urge to meet with others. Therefore, some of them celebrated parties in mainly unseen social spaces with a high degree of spreading of the infection.
In this respect, it is also apparent that the human being as a being is perceived too little in medicine, for example in the framework of a medical anthropology in the sense of Viktor von Weizsäcker. This also applies to other human sciences.
What is missing, therefore, is a holistic view of human beings as „situated subjects“ who, especially in this pandemic, cannot only be objects of administrative rationality. A framework of an „ecology of the human being“ or an „ecology of the person“ (human ecology) would be suitable for this purpose, which fundamentally considers the human being, his environment, and his relation to the environment as the object of consideration and as a guideline for a participatory design of measures (Tretter 2008 [35]).
Such a holistic-systemic view of the individual is also suitable for the sick person, seeing her as a bio-psycho-social being in the socio-ecological context. For this purpose, a person-centered systems medicine would be appropriate as a guiding model for medical thinking and acting.
The necessity of a „clinical systems medicine“
First of all, it must be noted that contemporary medicine is developing almost exclusively into the direction of „clinical molecular biology“ and is increasingly losing sight of the whole person with her illness and also her situation. Since the successful completion of the Human Genome Project, however, it has become clear that the analysis of the molecular building blocks of life must be complemented by efforts targeting a holistic view of the whole organism. Thus, „Systems Biology“ was born around 2000 (Kitano 2002[36]), which was further developed into „Systems Medicine“ or „Medical Systems Biology“ around 2005 Hood 2013 [37]). The combination of molecular biological technology, which investigates at the molecular level systems such as the genome, the transcriptome, the proteome, the metabolome, the epigenome, etc., combined with “complexity mathematics” (e.g. multivariate statistics, graph theory) should transform medicine into a personalized, predictive, preventive and participatory medicine (P4 medicine). Based on this, a biotechnological optimism was proclaimed the last years, which can also be found in „precision medicine“. However, several authors from the fields of biology, information sciences and philosophy of science doubt that the claim to be able to realize a much more effective medicine can be fulfilled even approximately (Vogt 2017 [38]; Green 2016 [39]).
Above all, it is overlooked that the reality of clinical-practical work in medicine relies on the good „pre-technological“ clinical competence, i.e. being able to listen to the patient’s history, to prepare an efficient anamnesis and to conduct the adequate physical examination. This medical literacy is increasingly being replaced by technical procedures, such as digitalization, in a technology-centered rather than a medically-centered manner. This is becoming increasingly apparent in education, research, and practice. (Tretter and Löffler-Stastka 2019a [40]). This parceling out of medicine must be contrasted with a so-called „organismic systems medicine“, where integration options are at stake (Tretter 2019 [41]). Such a concept can be supplemented by an ecological perspective (Tretter and Löffler-Stastka 2019b [42]).
With regard to the COVID-19 problem, the aim of this concept is to explicitly take into account the organism’s own dynamics and the complex and multilevel defense mechanisms, for instance regarding the immune system with organs, connections, cells and signaling molecules. Not only the causal factors should be captured theoretically, but this model should serve as a conceptual framework for adjusting therapy and prophylaxis (see Fig. 4). In this conception, the human being with his organ systems is in the center of attention. Here is the special focus on the respiratory system, which is primarily confronted with and influenced by SARS-CoV-2, and which penetrates step by step into the cells of the respiratory organs (and other organs) of the organism. From a structure-oriented system view, in the sense of an organismic compartment model, local defense mechanisms are already active (semi-circular dark gray lines with crossbars) when the virus enters the organism via the upper respiratory tract, which can weaken or even stop the viral invasion. In line with this concept, it is important to note that maybe 50 % of infected persons are aymptomatic cases as they were identified by representative serological studies and catamnestic observations (Nikolai et al. 2020 [43], Heneghan et al. 2020 [44]). In other words: the reported number of infected persons that were identified by testing must be doubled. In order to explain the high number of asymptomatic infected persons several hypotheses might fit. One of the most intriguing hypothesis proposes that the functionality of the micromilieu of the mucosa of the nose as a primary boundary structure for respiratory functions could be the crucial protector. It is well known now that the virus enters the cells via a special membrane-based enzyme that is important for inflammatory molecular and cellular processes (ACE2R; angiotensin converting enzyme 2). By this intervention of the virus the balance between pro-inflammatory and anti-inflammatory mechanisms is disturbed in favor of a dysfunctional persistence of pro-inflammatory activities which explains the clinically observed self-destructive hyperactivity of cytokines and lymphocytes. Interestingly, here the basic concept of a “dynamic flow equilibrium” within the renin angiotensin system (RAS) that is constituted by the metabolism of antagonistically organized angiotensin pathways and that exhibit a feedback loop to the kidneys could help to optimize medications in acute stages of COVID-19 infection: the virus reduces the anti-inflammatory activity of RAS and therefore the dominating angiotensin AT1 receptor-based pro-inflammatory pathway could be attenuated by AT1 receptor blocker and/or some enzyme blocker or by similar strategies (Lumbers et al. 2020 [45]). In addition, other endocrine loops such as the cortisol regulating loops that partially interfere with the IL-6 related control mechanism of the hypothalamus-pituitary-adrenal axis (HPA axis) have to be considered as dexamethasone is an effective late medication in severe courses of COVID-19. Finally, the activation level of the autonomous nervous system might be an important modulator of the functionality of the immune system as immune cells have noradrenergic receptors that attenuate or enforce the functions of macrophages, monocytes, Th cells etc. This is also true for parasympathetic inputs to the various immune cells.
These brief hints indicate that the invasion of the virus disturbs a preexisting dynamic balance of coupled autonomic nervous system, endocrine system and immune system that still has to be explored by appropriate experiments. These findings could contribute to the “big picture” of COVID-19 being able to explain various phenomena and to guide the development of effective and safe new medications for COVID 19.
In order to complete the big picture, the psychosocial determinants of health have to be considered additionally. For instance, the infected person may experience the disease through symptoms (double arrow) and/or obtain and use the knowledge about the virus and its prevention and treatment by the respective socio-cultural system at micro, meso and macro level. With this „mindset“, the person can change his or her behavior, depending on the social context, by reducing exposure behavior through distancing, quarantine, etc. (-) or through risky behavior (+) with corresponding consequences for the social environment. For instance, the exposure behavior might be risky with regard to the infection, but it also influences the distribution of the infection within the population. Also, the degree of access to health care units depends on the class affiliation of the respective person. These factors influence the individual and collective outcome of the management of COVID-19. On the other hand, the spread of the virus can also be caused by the spreading behavior of the person (heavy breathing, sneezing, singing, screaming, etc.).
This sketch of a person- and pathology-centered model is to a certain extent complementary to the socio-ecological system model in Figure 3, which depicts the society-centered macro level (see Figure 4). Research that examines both levels in relation to each other would be able to increase the coherence of the knowledge process to COVID-19 significantly. It also makes clear how many generic factors of the disease process are behind the epidemiological figures.

CONCLUSION
Here we aimed to show that a “systematic” application of multi-level systems thinking might help significantly to improve an integrated view of the COVID-19 problem. This kind of picture could guide scientific research in a more efficient way as it leads to more integrated questions regarding the optimal management of COVID 19. Basically, the epistemic object of COVID-19 research has to deal with a heterogeneous complex non-linear dynamic system that cannot be captured sufficiently by conventional methods of research.
[1] Bertalanffy …Bertalanffy, L.v. 1968. General System Theory. Braziller, New York
[2] Pueyo, T. 2020. Corona virus: The hammer and the dance. https://medium.com/@tomaspueyo/coronavirus-the-hammer-and-the-dance-be9337092b56
[3] Dammann O, Gray P, Gressens P, Wolkenhauer O, Leviton A. Systems Epidemiology: What’s in a Name? Online J Public Health Inform. 2014 Dec 15;6(3):e198. doi: 10.5210/ojphi.v6i3.5571. eCollection 2014.
[4] https://www.bcsss.org/de/research/fields-and-groups/systems-medicine-and-healthcare-systems/
[5] https://www.bcsss.org/de/2017/modeling-health-impacts-for-decision-making-on-status-and-perspectives/
[6] Meadows, D. H., Meadows, D. L., Randers, J., Behrens, W.W. (1972). The Limits to Growth; A Report for the Club of Rome’s Project on the Predicament of Mankind. New York: Universe Books.
[7] Tretter, F., Adam, D. 2020. COVID-19: Medizin, Politik und Öffentlichkeit. Wissenschaftstheoretische und -praktische Reflexionen. Berliner Ärzte 10/2020, 33-39
[8] Checkland P. Systems Thinking, Systems Practice. Chichester, England: John Wiley and Sons; 1981.
[9] Midgley G. Systemic Intervention: Philosophy, Methodology, and Practice. New York, NY: Kluwer Academic/Plenum Publishers; 2000.
[10] Maani KE, Cavana RY. Systems Thinking and Modelling: Understanding Change and Complexity. Auckland, New Zealand: Prentice Hall; 2000.
[11] Scholz, R.W. 2011. Environmental Literacy in Science and Society: From Knowledge to Decisions. Cambridge University Press, Cambridge
[12] Ison, R. 2020. The Hidden Power of Systems Thinking: Governance in a Climate Emergency. Routledge, London.
[13] Miller , J.G. 1978. Living Systems. New York: McGraw-Hill.
[14] Sterman, J. 2000. Business Dynamics. McGraw Hill.
[15] Sterman, J. 2006. Learning from Evidence in a Complex World. Am J Public Health. 2006 March; 96(3): 505–514. doi: 10.2105/AJPH.2005.066043, PMCID: PMC1470513, PMID: 16449579
[16] Midgley, G. Systemic Intervention for Public Health. April 2006. American Journal of Public Health 96(3):466-72. DOI: 10.2105/AJPH.2005.067660
[17] Tretter, F. 2000. Performance of health care units and the influence of management. In: Parra-Luna, F. (Ed): The Performance of social systems. Kluwer Academic, New York ,pp. 253-276
[18] Tretter, F. 2005. Krankes Gesundheitswesen und die Reformen – Kritik an der „politischen Gesundheitsökonomie“. Deutsches Ärzteblatt, 102(9): A- 570–571
Systemtheorie im klinischen Kontext. Pabst, Lengerich 2005
[19] Tretter, F. 2011. Systemisches Management im Gesundheitswesen. In: Kunhardt H. (eds) Systemisches Management im Gesundheitswesen. Gabler. https://doi.org/10.1007/978-3-8349-6440-3_2
[20] Schedler, K., Pröller, I. 2011. New Public Management. UTB, Haupt
[21] Tretter, F., Welpe, I.M. 2018. Krankenhaus-Management: Konzept für Paradigmenwechsel. Dtsch Arztebl 2018; 115(13): A-580 / B-504 / C-504
[22] Deutsches Ärzteblatt 2020b. MB-Monitor 2019: Ärzte fühlen sich überlastet. Dtsch Arztebl 2020; 117(5): A-186 / B-168 / C-164
[23] Antes, G. 2020. Die Zahlen sind vollkommen unzuverlässig. Spiegel online, 31.3.2020. www.spiegel.de/wissenschaft/medizin/coronavirus-die- zahlen-sind- vollkommen-unzuverlaessig-a-7535b78f-ad68-4fa9-9533-06a224cc9250 (abgerufen 01.07.2020).
[24] Network Evidence Based Medicine 2020. COVID-19: Wo ist die Evidenz? www.ebm-netzwerk.de
[25] Dörner, D. 1997. The Logic of Failure: Recognizing and Avoiding Error in Complex Situations. Basic Books, London
[26] Beer, S. 1972. Brain of the firm; a development in management cybernetics, New York, Herder and Herder
[27] Malik, F. 2008. Strategie des Managements komplexer Systeme: Ein Beitrag zur Management-Kybernetik evolutionärer Systeme. Haupt, Bern
[28] Tretter, F. 2011. Systemisches Management im Gesundheitswesen. In: Kunhardt H. (eds) Systemisches Management im Gesundheitswesen. Gabler. https://doi.org/10.1007/978-3-8349-6440-3_2
[29] Conover, C. 2020. How Economists Calculate The Costs And Benefits Of COVID-19 Lockdowns. Forbes March 27th
[30] Serbser, W. (Hrsg.) 2004. Humanökologie: Ursprünge – Trends – Zukünfte Edition Humanökologie Band 1, oekom Verlag, 2004
[31] Fischer-Kowalski, M. et al. (Hrsg.) 1997. Gesellschaftlicher Stoffwechsel und Kolonisierung von Natur. Ein Versuch in Sozialer Ökologie. Amsterdam
[32] Becker, E., Jahn, T. 2007. Soziale Ökologie. Campius, Frankfurt
[33] EU 2019a. Sustainable development in the European Union Monitoring report on progress towards the SDGs in an EU context. https://ec.europa.eu/eurostat/documents/3217494/9940483/KS-02-19-165-EN-N.pdf/1965d8f5-4532-49f9-98ca-5334b0652820
[34] EU 2019b. MITTEILUNG DER KOMMISSION AN DAS EUROPÄISCHE PARLAMENT, DEN EUROPÄISCHEN RAT, DEN RAT, DEN EUROPÄISCHEN WIRTSCHAFTS- UND SOZIALAUSSCHUSS UND DEN AUSSCHUSS DER REGIONEN: Der europäische Grüne Deal. https://ec.europa.eu/info/sites/info/files/european- green-deal-communication_de.pdf
[35] Tretter, F. 2008. Die Ökologie der Person. Pabst, Lengerich
[36] Kitano, H. 2002. Systems biology: a brief overview. Science 2002, 295:1662-1664
[37] Hood, L. 2013. Systems biology and p4 medicine: past, present, and future. Rambam Maimonides medical journal. 2013;4(2).
[38] Vogt, H. 2017. Systems Medicine as a Theoretical Framework for Primary Care Medicine. A Critical Analysis. Thesis for the Degree of Philosophiae Doctor Trondheim, Norwegian University of Science and Technology.
[39] Green, S. (Ed.) 2016. Philosophy of Systems Biology: Perspectives from Scientists and Philosophers [Internet]. Springer International Publishing;
[40] Tretter, F., Löffler-Stastka, H. 2019a. Medical knowledge integration and „systems medicine“: Needs, ambitions, limitations and options. September 2019 Medical Hypotheses 133:109386, DOI: 10.1016/j.mehy.2019.109386
[41] Tretter, F. 2019. “Systems medicine” in the view of von Bertalanffy’s “organismic biology” and systems theory. Res Behav Sci. 2019;36:346–362 Tretter, F. 2020. A systemic view on the corona crisis. www.bcsss.org/de/2020/a- systemic-view-on-the-corona-crisis-by-bcsss-vicepresident-felix- tretter/ (abgerufen 25.09.2020).
[42] Tretter, F., Löffler-Stastka, H. 2019b. The Human Ecological Perspective and Biopsychosocial Medicine.Int J Environ Res Public Health. 2019 Oct 31;16(21). pii: E4230. doi: 10.3390/ijerph16214230
[43] Nikolai L.A., Meyer C.G., Kremsner P.G., Velavan T.P. Asymptomatic SARS Coronavirus 2 infection: Invisible yet invincible.Int J Infect Dis. 2020; 100: 112-116
[44] Heneghan, C., Brassey, J., Jefferson, T. COVID-19: What proportion are asymptomatic? April 6, 2020
[45] Lumbers, E.R., Delforce, S.J., Kirsty G. Pringle, K.G, Smith, G.R. The Lung, the Heart, the Novel Coronavirus, and the Renin-Angiotensin System; The Need for Clinical Trials. Front. Med., 22 May 2020, https://doi.org/10.3389/fmed.2020.00248
Tretter, F. 2020. COVID-19 als Stresstest für die Wissensgesellschaft. MWV Berlin. https://www.mwv-berlin.de/meldung/!/id/310